Diabetes Quick Reference
Here you will find quick reference guides to help you diagnose and manage diabetes in your primary care practice with medication guidelines and cost information, as well as target benchmarks and management considerations for comorbid heart failure.
Ready to take the next steps to excellence in managing diabetes in primary care? Review the Mount Sinai Diabetes Care Pathway or discover services available to MSHP Clinically Integrated Network providers to achieve team-based care.
Download a print-friendly PDF of this guide

Diagnosing Prediabetes and Type 2 DM
Prediabetes
HbA1c between 5.7% – 6.4%
Fasting blood glucose between 100 – 125 mg/dl
An Oral Glucose Tolerance Test 2 hour blood glucose between 140 mg/dl – 199 mg/dl
Type 2 DM
A hemoglobin A1c (HbA1c) level of 6.5% or higher, or
A fasting plasma glucose (FPG) level of 126 mg/dL or higher
A 2-hour plasma glucose level of 200 mg/dL or higher during a 75-g oral glucose tolerance test (OGTT)
A random plasma glucose of 200 mg/dL or higher in a patient with classic symptoms of hyperglycemia or hyperglycemic crisis
Medications
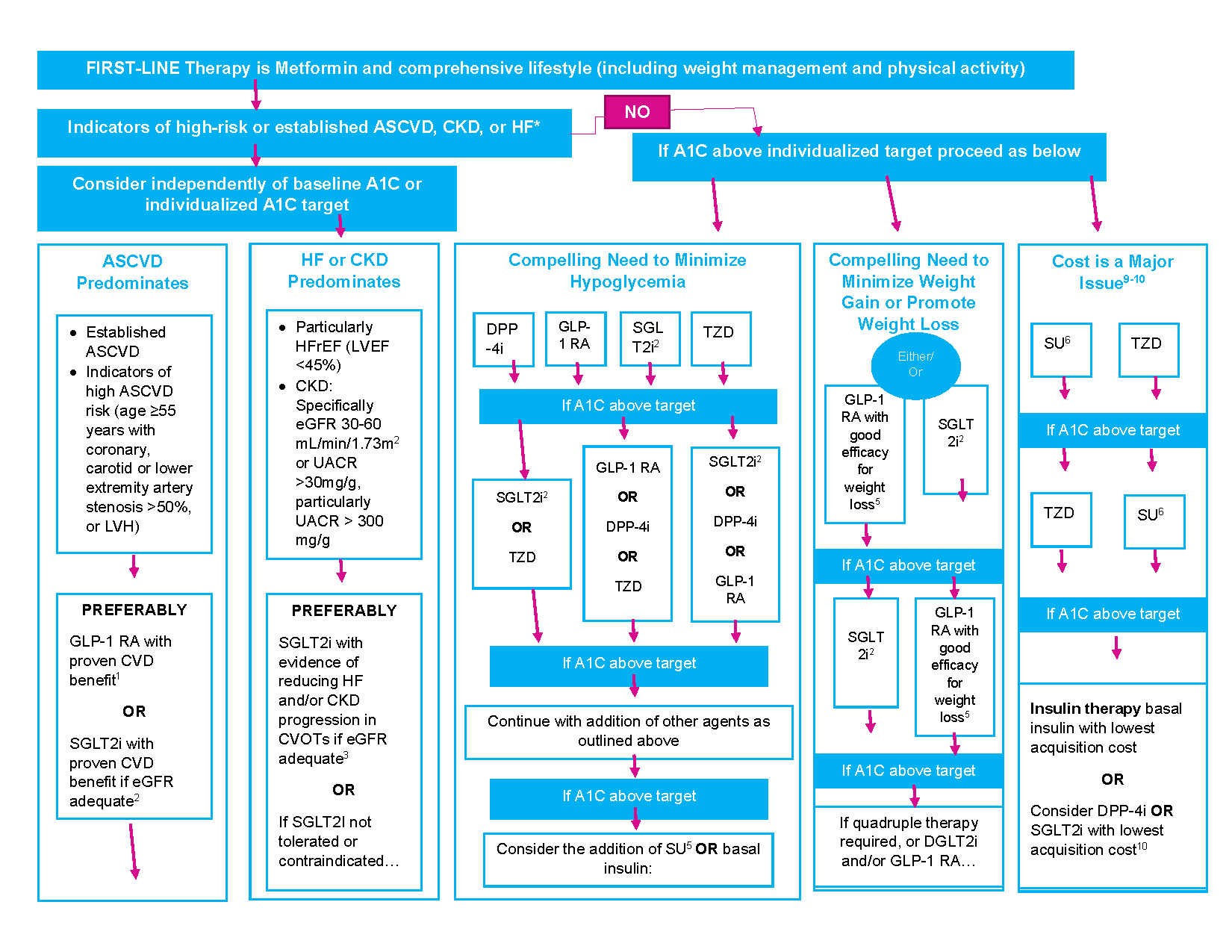
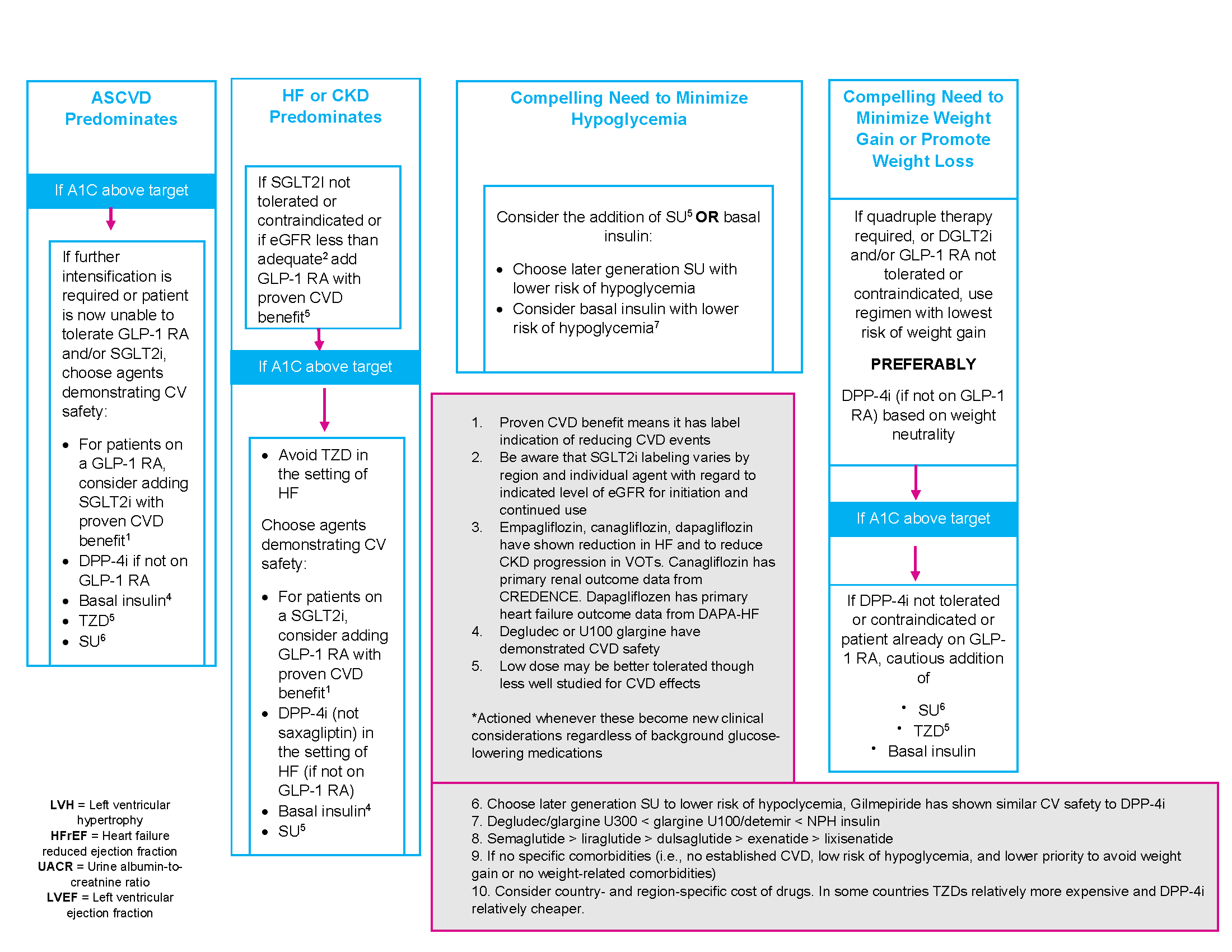
Oral Diabetes Medication Algorithm
Medication List, Dosing, & Cost
Anti-diabetic medication list median monthly (30-day) cost of maximum approved daily dose
Medication Class |
Compound(s) |
Common Trade Names |
Dosage strength/product (if applicable) |
Starting Dose (no renal/hepatic dysfuntion) |
Maxmimum approved daily dose* |
Median AWP (min, max)† |
|
Biguanides |
Metformin |
Glucophage Riomet |
500 mg (IR) |
500 mg qd |
2,000 mg |
$84 ($4, $85) |
|
850 mg (IR) |
2,550 mg |
$108 ($6, $109) |
||||
|
1,000 mg (IR) |
2,000 mg |
$87 ($4, $88) |
||||
|
Fortamet, Glucophage XR, Glumetza, Riomet ER |
500 mg (ER) |
500 mg qd |
2,000 mg |
$89 ($87, $7,412) |
||
|
750 mg (ER) |
1,500 mg |
$74 ($65, $74) |
||||
|
1,000 mg (ER) |
2,000 mg |
$242 ($242, $7,214) |
||||
|
Sulfonylureas (2nd generation) |
Glimepiride |
Amaryl |
1 mg, 2 mg, 4 mg |
1 mg qd |
8 mg |
$74 ($71, $198) |
|
Glipizide |
Glucotrol |
5 mg, 10 mg (IR) |
5 mg qd |
40 mg (IR) |
$75 ($67, $97) |
|
|
Glucotrol XL |
2.5 mg, 5 mg, 10 mg (XL) |
2.5 mg qd |
20 mg (XL) |
$48 |
||
|
Glyburide |
Glynase PresTabs |
1.5 mg, 3 mg, 6 mg (micronized) |
1.5 mg qd |
12 mg (micronized) |
$50 ($48, $71) |
|
|
None in USA |
1.25 mg, 2.5 mg, 5 mg |
2 mg qd |
20 mg |
$93 ($63, $103) |
||
|
Thiazolidinediones |
Pioglitazone |
Actos |
15 mg, 30 mg, 45 mg |
15 mg qd |
45 mg |
$348 ($283, $349) |
|
Rosiglitazone |
Avandia |
2 mg, 4 mg |
2 mg qd |
8 mg |
$407 |
|
|
Meglitinides (glinides) |
Nateglinide |
Starlix |
60 mg, 120 mg |
60 mg tid ac |
360 mg |
$155 |
|
Repaglinide |
Prandin |
0.5 mg, 1.0 mg, 2 mg |
0.5 mg tid ac |
16 mg |
$878 ($162, $897) |
|
|
DPP-4 inhibitors |
Alogliptin |
Nesina |
6.25 mg, 12.5 mg, 25 mg |
25 mg qd |
25 mg |
$234 |
|
Saxagliptin |
Onglyza |
2.5 mg, 5 mg |
5 mg qd |
5 mg |
$505 |
|
|
Linagliptin |
Trajenta |
5 mg |
5 mg qd |
5 mg |
$523 |
|
|
Sitagliptin |
Januvia |
25 mg, 50 mg, 100 mg |
100 mg qd |
100 mg |
$541 |
|
|
SGLT2 inhibitors |
Ertugliflozin |
Steglatro |
5 mg, 15 mg |
5 mg qd |
15 mg |
$338 |
|
Dapagliflozin |
Farxiga |
5 mg, 10 mg |
5 mg qd |
10 mg |
$591 |
|
|
Empagliflozin |
Jardiance |
10 mg, 25 mg |
10 mg qd |
25 mg |
$591 |
|
|
Canagliflozin |
Invokana |
100 mg, 300 mg |
100 mg qd |
300 mg |
$593 |
|
|
GLP-1 RAs |
Exenatide (extended release) |
Bydureon, Bydureon Bcise |
2 mg powder for suspension or pen |
2 mg qweek |
2 mg** |
$840 |
|
Exenatide |
Byetta |
5 mcg, 10 mcg pen |
5 mcg bid |
20 mcg |
$876 |
|
|
Dulaglutide |
Trulicity |
0.75mg, 1.5 mg, 3.0 mg, 4.5 mg |
0.75 mg qweek |
1.5 mg** |
$911 |
|
|
Semaglutide |
Ozempic |
0.5 mg, 1 mg pens |
0.25 mg qweek |
1 mg** |
$927 |
|
|
Rybelsus |
3 mg, 7 mg, 14 mg (tablet) |
3 mg qday |
14 mg |
$927 |
||
|
Liraglutide |
Victoza, Saxenda |
6 mg/ml, 18 mg/3 mL pen |
0.6 mg qweek |
1.8 mg |
$1,106 |
|
|
Lixisenatide |
Adlyxin |
300 mcg/3 mL pen |
10 mcg qday |
20 mcg |
$744 |
AWP, average wholesale price; DPP-4, dipeptidyl peptidase 4; ER and XL, extended release; GLP-1 RA, glucagon-like peptide 1 receptor agonist; IR, immediate release; N/A, data not available; SGLT2, sodium–glucose cotransporter 2.
†Calculated for 30-day supply (AWP) for dose highlighted and underlined in bold; median AWP listed alone when only one product and/or price.
*Utilized to calculate median AWP (min, max); generic prices used, if available commercially.
**Administered once weekly.
Management Targets
Screening/Management Target |
Benchmark |
Frequency |
Next Step if uncontrolled/positive finding |
Comments |
|---|---|---|---|---|
|
HgbA1c Test |
<7% |
Every 6 months if controlled Every 3 months if uncontrolled |
Lifestyle modification Escalate dosing of diabetes medication Referral to endocrinologist or pharmacist if HgbA1c >9% Care Management/Behavioral Health referral as indicated |
|
|
Blood Pressure Control |
BP <140/90 or <130/80 in select pts with CVD, CAD, or ASCVD risk > 15%* |
Annually if normal |
Lifestyle modification Home BP monitoring If no CKD, use ACE/ARB, diuretic, or CCB If CKD preent: ACE/ARB If resistant hypertension or progressive kidney disease, consider referral to nephrology or clinical pharmacy program |
|
|
Lipid Management |
LDL is <100 mg/dL With CV disease, target is <70 mg/dL. |
Annually |
Lifestyle modification Statin therapy |
|
|
Monitoring for Diabetic Kidney Disease (eGFR and UACR) |
eGFR >100 UACR <30 mg/g C |
Annually but consider semiannually if eGFR <60 or UACR > 30 mg/g of C |
ACE/ARB if eGFR <60 or UACR >30 Consider use of SGLT-2i or GLP-RA Intensify diabetes medications to optimize glycemic control Dietary intake of ~0.8g protein/kg weight per day Consider nephrology referral |
|
|
Retinopathy Screening |
Absence of retinopathy or macular edema |
If retinopathy or macular edema present, annual dilated eye exam or retinal photography |
Annual evaluation by ophthalmologist if retinopathy or macular edema present |
Screening can be performed in PCP office with a retinal camera; optometry clinic or ophthalmology clinic. |
|
Foot Exam |
No ulcerations or fungal infections, 2+ pedal pushes, normal sensory response with monofilament |
Annually |
Referral to podiatrist for management of any abnormalities Refer for Ankle Branchial Index (ABI) if Peripheral Arterial Disease (PAD) suspected |
Type 2 Diabetes and Heart Disease (Atherosclerotic Vascular Disease (ASVD) and Heart Failure (HF))
-
Ideally, risk factors for ASVD and Heart Failure should be assessed annually, using prognostic tools such as the ASCVD Risk Calculator. The 10 year risk of a first ASCVD event used to guide interventions.
-
Screening
-
Testing is indicated for typical/atypical chest pain, signs/symptoms of other vascular disease, or an abnormal ECG.
-
Exercise testing with/without echocardiography is the recommended initial test. Pharmacologic stress echo or nuclear imaging is indicated for those who are unable to exercise or have significant resting ECG abnormalities.
-
Routine screening for ASCVD with CT calcium scores/CT angiography in asymptomatic high risk patients is not recommended.
-
-
Antiplatelet Therapy
-
ASA (75-162 mg daily) may be used for primary prevention in diabetic patients aged 50-75 years with at least one additional ASCVD risk factors (family hx, dyslipidemia, hypertension, tobacco use, CKD/albuminuria) and not at increased risk of bleeding.
-
ASA (75-162 mg/d) maybe used for secondary prevention, in diabetic patients with known ASCVD (prior MI/stroke).
-
Clopidogrel may be used in patients with known ASA allergy.
-
-
In patients with known or multiple risk factors for ASCVD and/or CKD, an SGLT-2i or a GLP-1 RA should be part of the medication regimen.
-
Heart Failure
-
In patients with HF (with or without diabetes), a SGLT-2i may be used to reduce HF hospitalizations
-
Contraindicated:
-
DPP-4 Saxagliptin is associated with an increased risk hospitalization for HF and is contraindicated in HF patients.
-
Thiazolidinediones are also contraindicated in patients with heart failure
-
-
Next Steps
Read the Mount Sinai Diabetes Pathway for in-depth, evidence-based guidelines for managing your heart failure outpatients
Explore Team-Based Care services available to you and your practice as a member of MSHP's Clinically Integrated Network
Need a consult? Connect with our experts