COPD Quick Reference
Read on for information about commonly-prescribed medications and their indications, when to prescribe supplemental oxygen, clinical integration care delivery, and more.
Download a print-friendly PDF of this guide

Commonly Used Maintenance Medications in COPD
Generic Drug Name |
Inhaler Type |
Nebulizer |
Oral |
Injection |
Duration of Action | |
| Beta2-Agonists | ||||||
| Short-Acting (SABA) | ||||||
|
Levalbuterol |
MDI |
Yes |
6-8 hours |
|||
|
Albuterol |
MDI & DPI |
Yes |
Pill, syrup, extended release tablet |
Yes |
4-6 hours 12 hours (ext. release) |
|
|
Terbutaline |
DPI |
Pill |
Yes |
4-6 hours |
||
| Long-Acting (LABA) | ||||||
|
Formoterol |
DPI |
Yes |
|
|
12 hours |
|
|
Indacterol |
DPI |
|
24 hours |
|||
|
Olodaterol |
SMI |
|
24 hours |
|||
|
Salmeterol |
MDI & DPI |
|
|
|
12 hours |
|
| Anticholinergics | ||||||
| Short-Acting (SAMA) | ||||||
|
Ipratroplum bromide |
MDI |
Yes |
|
|
6-8 hours |
|
| Long-Acting (LAMA) | ||||||
|
Aclidinium bromide |
DPI & MDI |
|
|
|
12 hours |
|
|
Glycopyrronium bromide |
DPI |
|
Solution |
Yes |
12-24 hours |
|
|
Tiotropium |
DPI & SMI |
|
|
|
24 hours |
|
|
Umeclidium |
DPI |
|
|
|
24 hours |
|
| Combination Long-Acting Beta2-Agonist Plus Anticholinergic in One Device (LABA/LAMA) | ||||||
|
Formoterol/aclidium |
DPI |
|
|
|
12 hours |
|
|
Formoterol/glycopyrronium |
MDI |
|
|
|
12 hours |
|
|
Indacaterol/ glycopyrronium |
DPI |
|
|
|
12-24 hours |
|
|
Vilanterol /umeclidium |
DPI |
|
|
24 hours |
||
|
Olodaterol/tiotropium |
SMI |
|
|
|
24 hours |
|
| Methylxanthines | ||||||
|
Theophyline (SR) |
|
|
Pill |
Yes |
Variable, up to 24 hours |
|
| Combination of Long-Acting Beta2-Agonist Plus Corticosteroids in One Device (LABA/ICS) | ||||||
|
Formoterol/budesonide |
MDI & DPI |
|
|
|
12 hours |
|
|
Formoterol/mometasone |
MDI |
|
|
12 hours |
||
|
Salmeterol/fluticasone |
MDI & DPI |
|
|
|
12-24 hours |
|
|
Vilanterol/fluticasone furoate |
DPI |
|
|
|
24 hours |
|
| Triple Combination in One Device (LABA/LAMA/ICS) | ||||||
|
Fluticasone/umeclidium/vilanterol |
DPI |
|
|
|
|
|
| Phosphodietrase-4 Inhibitors | ||||||
|
Roflumilast |
|
Pill |
|
|
||
Abbreviations: FEV1, forced expiratory volume in 1 second; ICS , inhaled corticosteroids; LABA, long-acting ß2-agonist; LAMA, long-acting muscarinic receptor antagonist.
Reproduced with permission from the Global Initiative for Obstructive Lung Disease (GOLD), Global Strategy for the Diagnosis, Management and Prevention of COPD, 2017.
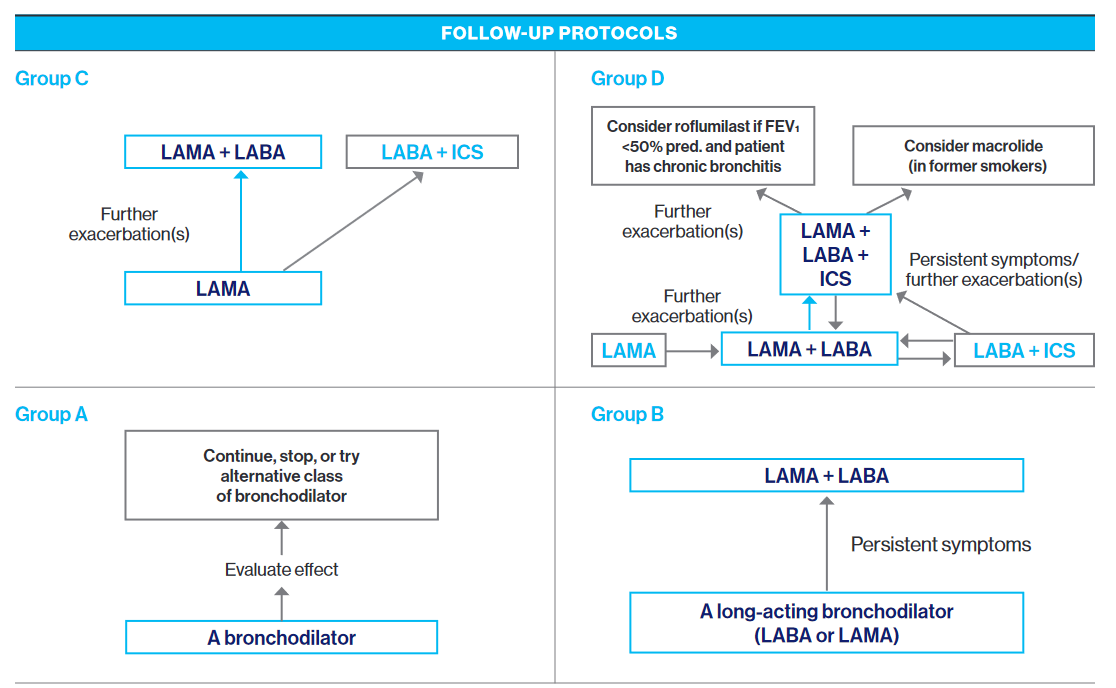
Pharmacologic Treatment Algorithms by GOLD Grade
APPROACH:
- Classify by GOLD Criteria using Modified Medical Research Council (MMRC), COPD Assessment Test (CAT), and # of exacerbations and hospitalizations.
- Patients must see a doctor at least four times (4x) per year for COPD management.
The Modified Medical Research Council (MMRC) Dyspnea Scale
Grade of Dyspnea |
Description |
|---|---|
|
0 |
Not troubled by breathlessness except on strenuous exercise |
|
1 |
Shortness of breath when hurrying on the level or walking up a slight hill |
|
2 |
Walks slower than people of the same age on the level because of breathlessness or has to stop for breath when walking at own pace on the level |
|
3 |
Stops for breath after walking about 100 m or after a few minutes on the level |
|
4 |
Too breathless to leave the house or breathless when dressing or undressing |
Source: Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest 1988; 93:580 - 586
COPD Assessment Test (CAT)
EXAMPLE |
I am very happy |
0 1 X 3 4 5 |
I am very sad |
|
I never cough |
0 1 2 3 4 5 |
I cough all the time |
|
|
I have no phlegm (mucus) on my chest at all |
0 1 2 3 4 5 |
My chest is full of phlegm (mucus) |
|
|
My chest does not feel tight at all |
0 1 2 3 4 5 |
My chest feels very tight |
|
|
When I walk up a hill or flight of stairs I am not out of breath |
0 1 2 3 4 5 |
When I walk up a hillor flight of stairs I am completely out of breath |
|
|
I am not limited to doing any activities at home |
0 1 2 3 4 5 |
I am completely limited to doing all activities at home |
|
|
I am confident leaving my home despite my lung condition |
0 1 2 3 4 5 |
I am not confident leaving my home at all because of my lung condition |
|
|
I sleep soundly |
0 1 2 3 4 5 |
I do not sleep soundly because of my lung condition |
|
|
I have lots of energy |
0 1 2 3 4 5 |
I have no energy at all |
TOTAL SCORE
Medication Guidelines (Groups A-D) Based on GOLD Classification
| INITIAL PHARMACOLOGICAL TREATMENTS | ||
|
At least 2 moderate exacerbations or at least 1 leading to hospitalization |
Group CLAMA |
Group DLAMA or LAMA + LABA* or ICS + LABA** *Consider if highly symptomatic (e.g. CAT >20) **Consider if eos is greater than or equal to 300 |
|
0 or 1 moderate exacerbations (not leading to hospitalization) |
Group AA bronchodilator |
Group BA long-acting bronchodilator (LABA or LAMA) |
|
Dyspnea scale 0-1, CAT <10 |
Dyspnea scale greater than or equal to 2, CAT greater than or equal to 10 |
|
Abbreviations: FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroids; LABA, long-acting ß2-agonist; LAMA, long-acting muscarinic receptor antagonist.
Reproduced with permission from the Global Initiative for Obstructive Lung Disease (GOLD), Global Strategy for the Diagnosis, Management and Prevention of COPD, 2017.
Non-Pharmacologic Management of COPD
| Patients Group | Essential | Recommended | Depending on Local Guidelines |
|
A |
Smoking cessation (can include pharmacologic treatment) |
Physical activity |
Flu vaccine Pneumococcal vaccine |
|
B-D |
Smoking cessation (can include pharmacologic treatment) Pulmonary rehabilitation |
Physical activity |
Flu vaccine Pneumococcal vaccine |
Prescription of Supplemental Oxygen to COPD Patients
-
Arterial hypoxemia defined as: PaO2 < 55 mmHg (8 kPa) or SaO2 < 88% or PaO2 > 55 but 60 mmHg (> 8 but < 8.5 kPa with right heart failure or erythrocytosis
-
Prescribe supplemental oxygen and titrate to keep SaO2 = 90%
-
Recheck in 60 to 90 days to assess:
-
If oxygen is still indicated
-
If prescribed supplemental oxygen is effective
-
Care Coordination in COPD at MSHS
-
Care Management
-
All patients should be evaluated by care management
-
Email mshpcmreferral@mountsinai.org or call 212-241-7228
-
Use the MSHP Care Management Referral in Epic (order #391414)
-
-
Behavioral Health
-
Patients should be screened for depression using the PHQ-2/PHQ-9 and referred to psychiatric services through their current care pathway depending on their clinic
-
-
Clinical Pharmacist
-
Pharmacists can be a key part of the care team for chronic disease management. They are credentialed providers that can prescribe and adjust medications through the Collaborative Drug Treatment Model
-
-
Palliative Care
-
Patients with COPD may be referred to one of two practices. The services provided at each location are identical; please choose the location that is most convenient to your patient
-
To make a referral to the Martha Stewart Center for Living at 1440 Madison Avenue, please call: 212-241-1446
-
To make a referral to the Martha Stewart Center for Living Downtown at Union Square, please call: 212-844-1712
-
-
Next Steps
Read the Mount Sinai COPD Pathway for in-depth, evidence-based guidelines for managing your COPD outpatients
Explore Team-Based Care services available to you and your practice as a member of MSHP's Clinically Integrated Network
Need a consult? Connect with our experts